
Ivermectin, Fenbendazole, Mebendazole, and Niclosamide for Cancer: Science, Real Stories & Protocols (2026 Guide)
Exploring the Science, Success Stories, and Protocols Behind Fenbendazole and Ivermectin in Cancer Research - Updated May 2026

In This Article:
Introduction
Chapter 1: Conventional, Standard Cancer Treatments and the Search for New Solutions
Chapter 2: Repurposing Existing Drugs for Cancer
Chapter 3: Ivermectin for Cancer
Ivermectin Mechanisms of Action in Cancer
Preclinical Evidence of Ivermectin (Cell and Animal Studies)
Ivermectin Clinical Evidence and Anecdotal Reports
Protocols and Dosing Strategies of Ivermectin
Chapter 4: Fenbendazole or Mebendazole for Cancer
Fenbendazole and Mebendazole Mechanisms of Action in Cancer
Preclinical Evidence of Fenbendazole and Mebendazole (Cell and Animal Studies)
Fenbendazole and Mebendazole Clinical Evidence and Anecdotal Reports
Protocols and Dosing Strategies of Fenbendazole and Mebendazole
Fenbendazole and Mebendazole Safety, Side Effects, and Toxicity
Chapter 5: Niclosamide for Cancer
Conclusion and Future Directions
Introduction
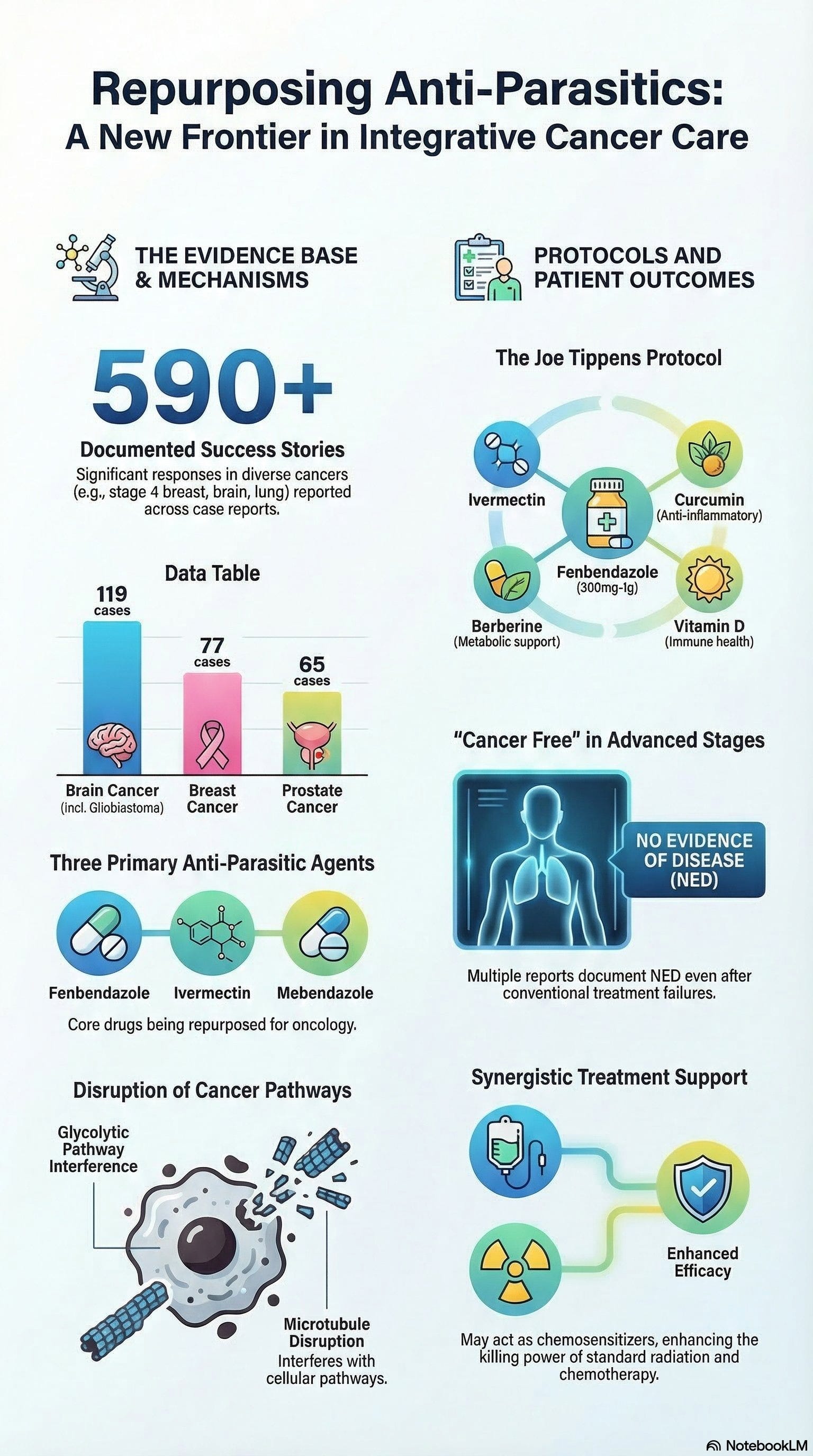
In 2016, Oklahoma businessman Joe Tippens was diagnosed with small-cell lung cancer, an aggressive form that had already metastasized to his pancreas, liver, bladder, bones, and neck. Given the extent of the spread, doctors gave him only a few months to live.
Facing this grim prognosis, Tippens learned from a veterinarian about fenbendazole, an antiparasitic drug used in animals. A scientist with terminal cancer had reportedly cured her lab mice—and herself—using this drug. With nothing to lose, Tippens decided to try fenbendazole alongside his conventional treatments.
The story was the beginning of what eventually became the “Joe Tippens Protocol.”
The Fenbendazole Cancer Protocol has been gaining rapid interest over the past years following some fenbendazole advanced cancer success stories.
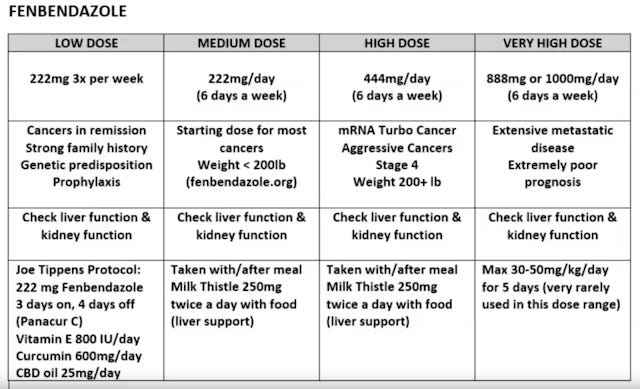
Fenbendazole, sold under the trade name Panacur, is available over the counter at veterinary supply stores but has not been approved by the U.S. Food and Drug Administration (FDA) for human use. Tippens began taking 1 gram per day for three consecutive days each week, cycling after four days off. Alongside fenbendazole, he supplemented with Theracurmin (a bioavailable form of curcumin) and CBD oil.
Remarkably, after three months, Tippens was declared cancer-free. His case gained widespread attention, sparking interest in fenbendazole’s potential as an adjunct cancer therapy. Tippens’ story inspired many others to explore fenbendazole and similar drugs like ivermectin, which have also been reported anecdotally to have anti-cancer effects.
This guide explores the scientific mechanisms behind these drugs’ potential to combat cancer. It examines how they might disrupt tumor growth, induce cancer cell death, or starve tumors of nutrients. Grounded in peer-reviewed research and supplemented with accessible explanations, this guide aims to clarify what might be happening inside the body when these unconventional treatments are used.
A balanced literature search reveals preliminary signals in small trials but emphasizes the need for rigorous validation to avoid misleading patients. Recent studies highlight ivermectin’s synergy with immune checkpoint inhibitors (immunotherapy) in breast cancer models and mebendazole’s combination with docetaxel in prostate cancer, underscoring repurposing potential. (Nature 2021, Nature 2019)
While the healing stories shared are anecdotal and not clinical proof, they raise important questions worthy of investigation. This work seeks to bridge the gap between compelling personal testimonies and scientific understanding in the ongoing search for effective cancer treatments.
Note for Clinicians:
Most supporting evidence comes from preclinical studies rather than randomized controlled trials (RCTs). This is partly because RCTs in this space are difficult to fund. Mainstream oncologists may dismiss this material as a result.
Importantly, many documented case reports involving patients with stage 4 cancers—who have undergone extensive prior treatments and lack actionable mutations for targeted therapies—have shown positive responses (complete response, partial response, or stable disease) to repurposed drugs such as ivermectin and mebendazole. This patient population generally has very limited treatment options. Referrals for second or third opinions to oncologists may not be fruitful, as many are unfamiliar with or untrained in the use of repurposed drugs within integrative oncology frameworks.
Clinicians should weigh potential benefits against risks, obtain informed consent, and consider referring to colleagues experienced in integrative oncology. Drug repurposing is a promising, cost-effective, and potentially lower-toxicity approach that warrants serious attention.
Chapter 1: Conventional, Standard Cancer Treatments and the Search for New Solutions
Cancer remains one of the world’s most significant health challenges, imposing a substantial burden in terms of new cases and mortality. In 2020, an estimated 19.3 million people worldwide were diagnosed with cancer, and approximately 10 million died from the disease that year. This makes cancer a leading cause of death globally, accounting for about one in six deaths overall.
Thanks to advances in early detection and treatment, survival rates have improved for many cancer types over recent decades. For example, in the United States, the overall 5-year survival rate for all cancers combined has increased from around 49% in the 1970s to roughly 68% for patients diagnosed in the 2010s. However, these improvements are not uniform across all cancer types or stages. Certain malignancies continue to have poor outcomes; pancreatic cancer, for instance, remains particularly lethal, with only about 12-13% of patients surviving five years after diagnosis. More broadly, once cancers have metastasized to distant organs, cure rates remain extremely low.
The persistent high mortality associated with advanced cancers underscores the urgent need for new solutions and strategies in oncology. Moreover, the global cancer burden is expected to rise sharply, with projections estimating over 35 million new cases by 2050—a 77% increase from 2022 figures. This growth reflects population aging, demographic changes, and evolving exposure to risk factors such as tobacco use, alcohol consumption, obesity, and environmental pollutants.
Despite progress in some regions, significant disparities in cancer incidence and outcomes persist both between and within countries. Access to early detection, quality treatment, and palliative care remains uneven, disproportionately affecting underserved populations. Addressing these inequities is critical to reducing the global cancer burden and improving survival for all patients.
Limitations of Standard Cancer Therapies
Modern oncology has made great strides with a toolkit of standard treatments which includes surgery, chemotherapy, radiation therapy, hormonal therapy, targeted drugs, and immunotherapy. These modalities have extended lives and even cured many early-stage cancers. Nevertheless, each standard treatment modality comes with significant limitations:
Chemotherapy: Cytotoxic chemotherapy drugs attack rapidly dividing cells to kill cancer, but "the downside is that it may also damage healthy cells in the process." This non-specific toxicity causes well-known side effects such as fatigue, nausea, hair loss, immune suppression, and organ damage. While chemo can shrink tumors, its lack of selectivity means normal tissues (bone marrow, gut lining, hair follicles, etc.) are harmed alongside cancer cells, limiting the doses patients can tolerate. Furthermore, cancers often develop resistance to chemotherapy over time, and chemo alone rarely eradicates advanced metastatic disease completely.
Radiation Therapy: High-energy radiation is very effective at killing cancer cells in a targeted area (for example, a tumor and its immediate surroundings). Technology has improved the precision of radiotherapy, yet it "can also affect surrounding healthy tissue". This collateral damage leads to side effects localized to the treatment field, such as skin burns, fibrosis, or damage to adjacent organs. Radiation is generally a local treatment and cannot reach cancer that has spread widely through the body. Thus, while it can cure or control localized tumors, it is less useful for widespread metastatic cancer except for palliative symptom relief. There is also a small risk that radiation itself can induce secondary cancers or other late complications years after treatment due to DNA damage in normal cells.
Immunotherapy: Over the past decade, immunotherapy (such as checkpoint inhibitor drugs and CAR-T cell therapy) has revolutionized treatment for some cancers by harnessing the patient’s own immune system to attack tumors. A subset of patients experience dramatic, long-lasting tumor regression from immunotherapies that would not respond to chemo or radiation. However, only about 20-40% of patients respond to current immunotherapy drugs. Many patients’ cancers do not react to immunotherapy at all, or they may initially respond but later relapse as tumors develop immune evasion mechanisms. Moreover, unleashing the immune system can trigger severe immune-related side effects; these range from mild (e.g., rash, fatigue) to life-threatening autoimmune reactions (e.g., colitis, hepatitis, endocrine disorders).
Immunotherapies are also extremely expensive, putting them out of reach in many healthcare settings. In short, while immunotherapy is a breakthrough for some, it is not yet a cure-all and leaves the majority of patients in need of other options.Even when standard treatments do achieve remission, cancer can recur in many cases. Microscopic cancer cells often survive initial therapy and later give rise to recurrence or metastasis. Thus, treatment of advanced cancer is often not definitively curative with current modalities. Patients and oncologists must balance the potential benefits of aggressive treatments with their toxicity and impact on quality of life. These limitations of the "tried-and-true" therapies have driven growing interest in supplementing conventional care with new approaches.
"Science is for all of us, not some of us"
Patient-Driven Demand for Adjunctive and Complementary Approaches
Facing the harsh side effects and the often incomplete success of standard cancer treatments, it’s no surprise that many patients start exploring other paths to support their healing. They’re not necessarily rejecting conventional medicine; they’re looking to complement it, to feel more in control, and maybe even tip the scales in their favor. In fact, surveys show that about 70% of cancer patients use some form of complementary or alternative medicine alongside their regular treatment.
A good example of this mindset is Steve Jobs. When he was diagnosed with a rare form of pancreatic cancer in 2003, he didn’t immediately follow his doctors’ advice to undergo surgery. Instead, he explored a range of alternative therapies including special diets, acupuncture, herbal remedies, and even spiritual practices. Jobs was someone known for thinking differently, and his approach to cancer reflected that. He wanted to do more than just follow a medical script. He wanted to pursue every possible option, even those outside the mainstream, to try and regain some sense of control over the situation.
Like Jobs, many patients turn to a wide variety of adjunct therapies such as nutritional supplements, mind-body practices like meditation or yoga, and off-label drugs not typically used for cancer. Some do it to ease the side effects of chemo or radiation. For example, they might use acupuncture to reduce nausea or meditation to calm the mind. Others, especially those with advanced or recurring cancer, are hoping these therapies might slow the cancer down, boost their body’s natural defenses, or just help them feel a little better day to day. It’s a deeply human response: when the road is hard and uncertain, people look for every bit of light they can find. The desire for a sense of control also plays a role as exploring integrative therapies allows patients to take an active role in their care rather than relying solely on hospital treatments.
Crucially, many are inspired by anecdotal success stories shared in patient communities and online forums, where individuals claim that various unconventional remedies helped them achieve remission or improved their well-being. This peer-to-peer influence has grown in the internet and social media era, accelerating the popularity of certain adjunct treatments. However, it also raises concerns, as not all “cancer cure” claims are credible and some unproven remedies can interfere with standard care. The strong patient demand for adjunctive options sends a clear message: there are gaps in current cancer therapy that patients desperately want to fill, whether it be reducing toxic side effects, addressing treatment-resistant disease, or preventing recurrence.
Chapter 2: Repurposing Existing Drugs for Cancer
Cancer remains a leading cause of morbidity and mortality worldwide, with an increasing incidence of aggressive and treatment-resistant tumors such as triple-negative breast cancer (TNBC), pancreatic adenocarcinoma, and glioblastoma. Despite significant advances in targeted therapies and immunotherapies, many patients continue to face limited effective options, highlighting an urgent need for novel, affordable, and accessible treatment strategies.
There is a reason that cancer rates are rising to become the number one cause of death in developed and Western countries. Our current cancer system works well if one has an early disease. The cure rates and survival are generally excellent. The lesion is removed, and so long as the tumor has not spread, that may be the end of it. The problem comes with advanced disease. When dealing with stage 4 cancer, those that have spread and seeded distant locations, the chances of cure drop. The chances of toxicity rise. At this point, the patient often dies, either from cancer itself or from complications of the treatment.
Why do we accept this reality? Why have we not adopted less toxic therapy that is known to prevent tumor resistance, and metastatic spread, as it exists in the form of repurposed drugs? Perhaps it is because, in the early days of treating cancer, there was no alternative other than death. Our cancer care treatment protocols have not kept pace with technology.
Today, we have targeted immunotherapy. We have precise radiation beams. Most importantly, through our genetic knowledge of tumors, we have existing drugs that can prevent resistance by targeting key cancer stem cell pathways.
We have sequenced the genome. But we have not yet applied this knowledge in treating terminal cancer. We still treat terminal cancer patients with the old protocols of 50 years ago-surgery, chemotherapy, and radiation.
The high cost of oncology drugs-exceeding $150 billion globally in 2022-and the slow pace of new drug approvals further complicate timely patient access to effective therapies. In this context, drug repurposing-the strategy of identifying new therapeutic uses for existing drugs-has emerged as a promising approach to accelerate cancer treatment development while reducing costs and safety risks.
Is it legal for doctors to prescribe drugs for treating disease beyond their approved purposes? The answer is yes. Medical doctors can legally prescribe drugs for uses beyond their approved purposes, a practice known as off-label prescribing. However, laws and regulations regarding this vary by country, and it is essential to confirm the specifics with a local doctor or legal expert in your jurisdiction. Off-label use is often based on clinical judgment when doctors believe that an unapproved use may benefit the patient, especially in cases where approved treatments are limited. While common, this practice requires careful consideration of evidence, potential risks, and patient consent to ensure safety and appropriateness.
The Mebendazole Discovery
For anyone who has not learned of Dr. Gregory Riggins and his chance discovery of a cure for cancer, the story goes like this (Justus Hope 2020):
In 2011, Dr. Gregory Riggins, a neurosurgeon at Johns Hopkins University, had given his mice cancer. By carefully implanting malignant cells from a live tumor into each of their brains, they would now all grow brain medulloblastomas. New drugs and human cancer treatments could be tested.
But before the experiment could begin, his mice came down with a bad case of worms. Dr. Riggins did what any good scientist would:
He treated them with a pinworm drug. Following the deworming treatment, the mice were once again healthy and worm-free, but quite inexplicably they were also cancer-free.”
After the mice got the pinworm drug, Dr. Riggins reported, “Our medulloblastomas stopped growing.”
Riggins began studying the pinworm drug he gave them, mebendazole (or MBZ, for short) as an anticancer treatment. Mebendazole has been used safely for 40 years to treat parasites.
Preliminary results showed MBZ to be effective at treating a large variety of cancers, including leukemia, lymphoma, lung cancer, colon cancer, and brain cancers such as glioblastoma and medulloblastoma.
Compared to vincristine, the current standard treatment for pediatric brain tumors, MBZ is relatively safe, and nontoxic. Vincristine is old school chemo, replete with side effects such as nausea, vomiting, hair loss, and immune suppression. Both vincristine and mebendazole work by blocking microtubule assembly in cells.
The Care Oncology Clinic in the UK, which is now doing clinical trials on glioblastoma, published their preliminary retrospective data from the METRICS study (NCT02201381) in Frontiers in Pharmacology (2019) about the combination standard treatment and repurposed drugs in 95 patients. Simply adding metformin, doxycycline, atorvastatin, and mebendazole can increase GBM (Glioblastoma) average survival from 15 to 27 months, almost a doubling.
Antiparasitic Drugs as Cancer Agents
Among repurposed candidates, antiparasitic drugs such as fenbendazole, mebendazole, ivermectin and most recently, niclosamide; have attracted considerable attention due to their demonstrated anticancer activities across multiple preclinical models and emerging clinical case reports. These agents, originally developed to treat helminth infections, exert multifaceted effects on cancer cells, including disruption of microtubule dynamics, interference with metabolic pathways, and modulation of oncogenic signaling.
Fenbendazole disrupts microtubule assembly, arrests the cell cycle at G2/M phase, and impairs glucose metabolism by blocking GLUT1/4 transporters and hexokinase — effectively starving cancer cells that rely on glycolysis (the Warburg effect). It has also shown efficacy against chemotherapy-resistant cell lines.
Mebendazole shares fenbendazole’s core mechanisms but offers better oral bioavailability and a longer history of human use. It crosses the blood-brain barrier, making it particularly relevant for brain tumors. Clinical trials in gastrointestinal cancers and pediatric brain tumors have been conducted, with pharmacokinetic challenges noted.
Ivermectin works differently — through a broader set of molecular targets including STAT3, Wnt/β-catenin, and AKT/mTOR pathways. It induces apoptosis, autophagy, and oxidative stress in cancer cells while also targeting cancer stem cells and modulating the tumor microenvironment. It has demonstrated activity across more than 20 cancer types in preclinical studies.
Niclosamide is an FDA-approved antihelminthic drug with one of the broadest oncogenic pathway profiles of any repurposed agent. It inhibits Wnt/β-catenin, STAT3, mTORC1, NF-κB, and Notch signaling simultaneously while acting as a mitochondrial uncoupler — disrupting cancer cell energy production from two directions at once. It is also among the most potent inhibitors of cancer stem cells identified to date. Its primary clinical limitation is poor oral bioavailability, which ongoing formulation research is working to address.
Despite encouraging preclinical and anecdotal clinical evidence, these antiparasitic agents remain largely experimental in oncology, with limited randomized controlled trials* and regulatory approval for cancer indications. Variability in dosing protocols, access issues, and concerns about off-label use underscore the need for rigorous clinical evaluation. Nonetheless, their low cost, oral administration, and multi-targeted anticancer properties position fenbendazole, mebendazole, and ivermectin as attractive candidates for adjunctive cancer therapy, especially in resource-limited settings.
*Note: The RCT is the gold standard for medical evidence — but it is poorly suited to the complexity of cancer biology. Most drugs are designed to affect one part of cancer and not the other parts of cancer or even the root causes of cancer. To understand more of this concept, check out 'hallmarks of cancer'. The randomized placebo-controlled trial (RCT)* is widely regarded as the gold standard for generating high-quality evidence in medicine. However, when it comes to cancer, the RCT model is often prohibitively expensive, time-consuming, and sometimes impractical. See "Randomised controlled trials (RCTs), are often costly, slow, and logistically challenging - ChatGPT".
Related: Top 20 Alternative Cancer Treatments that Work: Evidence Based (2025 Edition)
Chapter 3: Ivermectin for Cancer
Ivermectin Mechanisms of Action in Cancer
Ivermectin, originally discovered as a potent antiparasitic agent, has garnered significant scientific interest for its potential anti-cancer properties. Since its FDA approval in 1987 for treating parasitic infections such as onchocerciasis, ivermectin has been administered to nearly 250 million people annually with minimal side effects. Beyond its antiparasitic role, extensive preclinical research has demonstrated ivermectin’s ability to target a wide range of cancers—over 20 types have shown susceptibility in laboratory and animal studies.
Despite these promising findings, ivermectin's transition into clinical oncology remains limited. This is largely due to its off-patent status and low cost, which reduce pharmaceutical incentives for costly clinical trials.
This chapter explores the current landscape of ivermectin research in oncology, detailing its multifaceted mechanisms of action, the cancers it may target, and the clinical implications of these findings.
Ivermectin’s Anti-Cancer Mechanisms: An Overview
Ivermectin exerts anti-cancer effects through multiple pathways, targeting both tumor cells and the tumor microenvironment. Its mechanisms include:
Inhibition of Cancer Cell Proliferation: Ivermectin disrupts key signaling pathways such as Akt/mTOR, Wnt/β-catenin, and MAPK, which are critical for cancer cell growth and survival.
Induction of Tumor Cell Death: It promotes various forms of cell death including apoptosis (programmed cell death), autophagy (cellular self-digestion), and pyroptosis (inflammatory cell death).
Targeting Cancer Stem Cells: By inhibiting cancer stem cells, ivermectin may prevent tumor initiation, progression, and recurrence.
Modulation of Tumor Microenvironment: It enhances immunogenic cell death (ICD) via pathways like P2X7, potentially improving immune recognition of tumors.
Inhibition of Metastasis: Through suppression of PAK1 and RNA helicase activity, ivermectin reduces cancer cell migration and invasion.
Mitochondrial Dysfunction: Ivermectin impairs mitochondrial biogenesis and function, increasing reactive oxygen species selectively in cancer cells.
Anti-Angiogenic Effects: It inhibits the formation of new blood vessels that tumors require for growth.
Epigenetic Regulation: Ivermectin modulates gene expression via SIN3 domain interactions, restoring sensitivity to therapies like tamoxifen.
Overcoming Multi-Drug Resistance (MDR): It enhances the efficacy of chemotherapeutic agents and reduces resistance development.
These mechanisms have been validated across numerous in vitro (cell culture) and in vivo (animal) studies, often at concentrations achievable in humans. See references: Ivermectin’s Anti-Cancer Mechanisms.
Molecular Targets and Pathways of Ivermectin in Cancer
A detailed look at ivermectin’s molecular targets reveals the following key pathways and their associated cancers:
Akt/mTOR Pathway
Cancer Types: Glioblastoma, renal cancer, leukemia
Mechanism: Inhibits mitochondrial function, induces oxidative stress and DNA damage.
Wnt/β-catenin Pathway
Cancer Types: Glioblastoma, colon cancer, melanoma, breast, skin, lung cancers
Mechanism: Inhibits proliferation and formation of cancer stem cells.
PAK1 (p21-activated kinase 1)
Cancer Types: Glioblastoma, ovarian cancer, breast cancer, lung cancer
Mechanism: Promotes autophagy, inhibits cancer cell migration and invasion.
P2X7 Receptor (Immunogenic Cell Death - ICD)
Cancer Types: Triple-negative breast cancer
Mechanism: Enhances immune-mediated tumor cell death.
SIN3 Domain (Epigenetic Regulation)
Cancer Types: Breast cancer
Mechanism: Modulates gene expression and restores sensitivity to therapies like tamoxifen.
NS3 Helicase
Cancer Types: Glioma
Mechanism: Inhibits RNA helicase activity, reducing cancer cell proliferation and invasion.
YAP1 (Yes-associated protein 1)
Cancer Types: Hepatocellular carcinoma, cholangiocarcinoma, colorectal, ovarian, gastric cancers
Mechanism: Suppresses tumor progression.
Mitochondrial Dysfunction
Cancer Types: Multiple cancers including glioblastoma, leukemia
Mechanism: Inhibits mitochondrial biogenesis and respiration, increases reactive oxygen species selectively in cancer cells.
Angiogenesis Inhibition
Cancer Types: Various
Mechanism: Blocks formation of new blood vessels essential for tumor growth.
Multi-Drug Resistance (MDR) Overcoming
Cancer Types: Various
Mechanism: Enhances chemosensitivity and reduces drug resistance.
See references: Ivermectin’s Anti-Cancer Mechanisms.
Preclinical and Emerging Clinical Evidence of Ivermectin for Cancer
In Vitro and In Vivo Studies (Pre-clinical)
Ivermectin has demonstrated anti-cancer activity in cell lines and animal models of:
Bladder Cancer - (2024 Fan et al) - Ivermectin Inhibits Bladder Cancer Cell Growth and Induces Oxidative Stress and DNA Damage.
Breast Cancer - (2018 Dominguez-Gomez et al) - Ivermectin as an inhibitor of cancer stem-like cells.
Brain Cancer - (2016 Liu et al) - Anthelmintic drug ivermectin inhibits angiogenesis, growth and survival of glioblastoma through inducing mitochondrial dysfunction and oxidative stress.
Bile Duct Cancer - (2019 Intyuod et al) - Anti-parasitic drug ivermectin exhibits potent anticancer activity against gemcitabine-resistant cholangiocarcinoma in vitro
Blood Cancer - (2020, de Castro et al) - Continuous high-dose ivermectin appears to be safe in patients with acute myelogenous leukemia and could inform clinical repurposing for COVID-19 infection.
Bone Cancer - (2022 Hu et al) - Repurposing Ivermectin to augment chemotherapy’s efficacy in osteosarcoma
Colon Cancer:
2022, Alghamdi et al - Efficacy of ivermectin against colon cancer induced by dimethylhydrazine in male wistar rats.
2025 Asano et al - Selective Synergy of Ivermectin Combined With Recombinant Methioninase Against Colon-Cancer Cells in Contrast to Normal Fibroblasts
Cervical Cancer - (2022, Qabbus et al) - Ivermectin-induced cell death of cervical cancer cells in vitro a consequence of precipitate formation in culture media
CML (Chronic Myeloid Leukemia) - (2018 Wang et al) - Antibiotic ivermectin selectively induces apoptosis in chronic myeloid leukemia through inducing mitochondrial dysfunction and oxidative stress.
Lung Cancer - (2024 Man-Yuan Li et al) - Ivermectin induces nonprotective autophagy by downregulating PAK1 and apoptosis in lung adenocarcinoma cells
Glioma - (2024 Xing Hu et al) - Ivermectin as a potential therapeutic strategy for glioma
Multiple Myeloma - (2024 Yang Song et al) - Gene signatures to therapeutics: Assessing the potential of ivermectin against t(4;14) multiple myeloma
Ovarian Cancer - (2023 Jawad et al) - Ivermectin augments the anti-cancer activity of pitavastatin in ovarian cancer cells
Prostate Cancer - (2022 Lu et al) - Integrated analysis reveals FOXA1 and Ku70/Ku80 as targets of ivermectin in prostate cancer
Pancreatic Cancer:
2022 Lee et al- Ivermectin and gemcitabine combination treatment induces apoptosis of pancreatic cancer cells via mitochondrial dysfunction.
2025 Morinaga et al - Ivermectin Combined With Recombinant Methioninase (rMETase) Synergistically Eradicates MiaPaCa-2 Pancreatic Cancer Cells.
Melanoma - (2022 Zhang et al) - Drug repurposing of ivermectin abrogates neutrophil extracellular traps and prevents melanoma metastasis
Liver Cancer - (2022 Lu et al) - Ivermectin synergizes sorafenib in hepatocellular carcinoma via targeting multiple oncogenic pathways
Stomach Cancer - (2021 Rabben et al) - Computational drug repositioning and experimental validation of ivermectin in treatment of gastric cancer
Esophagus Cancer - (2020, Chen et al) - Ivermectin suppresses tumour growth and metastasis through degradation of PAK1 in oesophageal squamous cell carcinoma
Kidney Cancer - (2017 Zhu et al) - Antibiotic ivermectin preferentially targets renal cancer through inducing mitochondrial dysfunction and oxidative damage
Animal studies have shown tumor volume reductions ranging from 50% to 85% depending on cancer type and dosing.
Clinical Evidence and Case Reports
As of 2026, formal clinical trials remain limited but are growing:
Phase II Trial (Yuan Yuan et al., 2025): Evaluating ivermectin combined with balstilimab in metastatic triple-negative breast cancer.
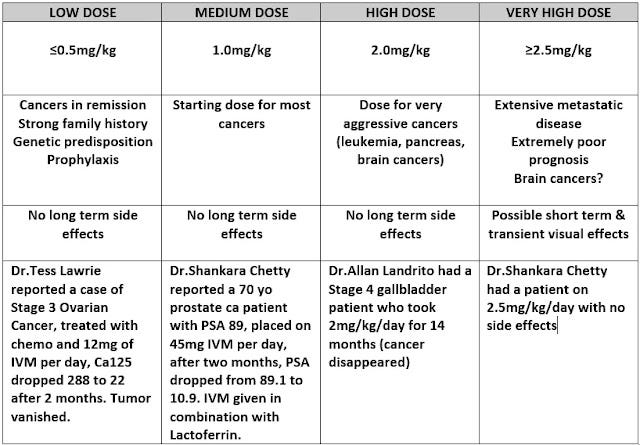
Case Reports: Anecdotal evidence suggests dramatic tumor marker reductions in advanced colon, ovarian, gallbladder, and prostate cancers with high-dose ivermectin regimens (up to 2 mg/kg daily).
Ivermectin, Fenbendazole, and Mebendazole for Stage 4 Cancer: More than 300 Case Reports Compilation
Fenbendazole Cancer Success Stories: More than 700 Case Reports Compilation (2026 Edition)
Triple combination of Ivermectin, Mebendazole and Fenbendazole for Cancer: 19 Case Reports (2026)
No serious adverse effects have been reported in healthy volunteers at doses up to 2 mg/kg, supporting ivermectin's safety margin for exploration in oncology settings.
Potential Clinical Applications and Dosing Considerations
Ivermectin’s broad anti-cancer potential suggests it may be especially useful against cancers with limited treatment options or those exhibiting drug resistance. Notably, cancers reportedly accelerated or “turbocharged” following COVID-19 mRNA vaccination—such as lymphomas, brain tumors (glioblastoma), triple-negative breast cancer, colon, lung, hepatobiliary, and melanoma—may benefit from ivermectin-based therapies.
Dosing:
Safe dosing in humans has been established up to 2 mg/kg orally, with peak plasma concentrations reached approximately 4 hours post-administration and a half-life of about 18–19 hours.
Anti-cancer effects appear dose-dependent, with higher doses correlating with improved responses.
Anecdotal regimens include daily or every-other-day dosing at or near 2 mg/kg for advanced cancers.
Combination Therapy:
Ivermectin shows synergistic effects when combined with chemotherapy agents such as paclitaxel and gemcitabine, potentially overcoming resistance and enhancing efficacy.
Drug interaction warning: Ivermectin significantly amplifies the anticoagulant effect of warfarin (Coumadin) and may interact with other blood thinners. Patients on anticoagulants should be closely monitored by a physician before and during use.
Chapter 4: Fenbendazole and Mebendazole for Cancer Therapy
Fenbendazole’s Anti-Cancer Mechanisms of Action
Fenbendazole (often abbreviated as fenben*) is a veterinary antiparasitic medication widely used to treat parasitic worm infections in animals, including tapeworms, hookworms, roundworms, and whipworms. Commonly marketed under brand names such as Panacur C and Safe-Guard, fenbendazole belongs to the benzimidazole class of anthelmintics, a group of drugs that includes mebendazole, albendazole, and flubendazole. While fenbendazole is approved only for veterinary use, mebendazole has been approved for human use to treat intestinal parasitic infections.
*Note: Yes, Fenben is the brand name for the active ingredient fenbendazole. (source)
In recent years, fenbendazole and mebendazole have attracted scientific and public attention for their potential anti-cancer properties. Both drugs exhibit multiple mechanisms that may inhibit cancer cell growth and survival, with studies demonstrating effectiveness against aggressive cancers such as triple-negative breast cancer, colon cancer, glioma, and leukemia. The ketogenic diet has also been suggested to enhance the therapeutic effects of these drugs.
Fenbendazole has been shown to exert anti-cancer effects through at least 12 distinct mechanisms, including:
Microtubule Disruption: Fenbendazole destabilizes microtubules, essential for cell division, leading to mitotic arrest and apoptosis in cancer cells.
Inhibition of Glucose Metabolism: It downregulates glucose transporters (such as GLUT1) and hexokinase II (HKII), starving cancer cells that rely heavily on glycolysis (the Warburg effect).
Induction of Apoptosis and Pyroptosis: Fenbendazole activates programmed cell death pathways, including caspase-mediated apoptosis and gasdermin-mediated pyroptosis, contributing to tumor cell elimination.
Oxidative Stress and Ferroptosis: It increases reactive oxygen species (ROS), promoting ferroptosis and enhancing cancer cell death.
Cell Cycle Arrest: Fenbendazole induces G2/M phase arrest, halting cancer cell proliferation.
Proteasomal Inhibition: It impairs proteasome function, disrupting protein degradation pathways vital for cancer cell survival.
Immune Modulation: Fenbendazole may influence the tumor microenvironment, enhancing anti-tumor immune responses.
Inhibition of Drug-Resistant Cells: It has shown efficacy against chemotherapy-resistant cancer cells, including those resistant to 5-fluorouracil and paclitaxel.
These mechanisms have been demonstrated across multiple cancer types, including lung, ovarian, colorectal, cervical, breast, and lymphoma models, both in vitro and in vivo.
Preclinical and Emerging Clinical Evidence
Several recent studies have explored fenbendazole’s anti-cancer potential:
In Vitro and Animal Studies: Fenbendazole reduces tumor volume in lung cancer xenografts and induces apoptosis in colorectal and breast cancer cells. It also inhibits glucose uptake and glycolysis, effectively starving tumor cells.
Case Reports: Anecdotal evidence from over 180 cancer patients using fenbendazole (often combined with ivermectin) reports tumor regression and improved outcomes, though these lack controlled clinical validation.
Ivermectin, Fenbendazole, and Mebendazole for Stage 4 Cancer: More than 300 Case Reports Compilation
Fenbendazole Cancer Success Stories: More than 700 Case Reports Compilation (2026 Edition)
Peer-reviewed Case Series: Fenbendazole as an Anticancer Agent? A Case Series of Self-Administration in Three Patients (2025 Case Reports in Oncology)
Combination Therapies: Research suggests fenbendazole may synergize with other agents like cetuximab and ketogenic diets to enhance anti-cancer efficacy.
Clinical Trials: While fenbendazole itself lacks extensive clinical trials in humans, mebendazole—its human-approved counterpart—has been studied in multiple clinical trials for various cancers, including brain tumors and gastrointestinal cancers.
Mebendazole: The Human-Approved Counterpart
Mebendazole (MBZ) shares chemical and pharmacological properties with fenbendazole but is FDA-approved for human use against parasitic infections. First introduced in the 1970s, mebendazole has since been repurposed in research as a potential anti-cancer agent.
Key findings include:
Triple-Negative Breast Cancer: Studies show mebendazole prevents tumor growth and metastasis by reducing cancer stem cells.
Pancreatic Cancer: Research from Johns Hopkins University advocates for mebendazole as an adjuvant therapy to slow progression and prevent recurrence.
Brain Tumors: Mebendazole crosses the blood-brain barrier, reaching therapeutic concentrations in brain tumors.
Clinical Trials: Phase 1 and 2 trials have explored mebendazole’s safety and efficacy in advanced gastrointestinal cancers and pediatric brain tumors, though challenges with drug absorption and serum levels have been noted.
Fenbendazole vs. Mebendazole: Differences and Considerations
Approval and Use: Mebendazole is FDA-approved for human use; fenbendazole is approved only for veterinary use.
Cost: Fenbendazole is significantly less expensive than mebendazole, making it attractive for off-label use.
Clinical Evidence: Most clinical data and trials focus on mebendazole, while fenbendazole’s evidence is primarily preclinical and anecdotal.
Efficacy: Some studies suggest mebendazole may be more effective against certain cancers such as brain, prostate, and ovarian cancers.
Fenbendazole and Mebendazole Dosing Protocols
Fenbendazole Dosing Protocols: Intermittent dosing (e.g., 3 days on, 4 days off) is often recommended to reduce liver stress, though some users tolerate daily dosing.
Mebendazole dosing in cancer trials varies widely, from 100 mg twice daily to doses as high as 4 g per day, with higher doses generally well tolerated. However, some trials have reported limited clinical responses, possibly due to pharmacokinetic limitations.
Fenbendazole and Mebendazole Safety, Side Effects, and Toxicity
Fenbendazole for humans is considered safe because of its low toxicity and high safety margin, as indicated by limited studies. However, it is important to remember that the FDA has not approved it. To determine the proper dosage of Fenbendazole for humans, studies have shown that a single oral dose of up to 2,000 mg per person or multiple doses of 500 mg per person for 10 days are generally safe. It’s important to note that these are only general guidelines, and the appropriate dosage may vary depending on each person’s specific cancer.
According to the product description on Amazon, fenbendazole is "Safe for all Dogs 6 weeks and older, including pregnant Dogs".
Based on toxicology studies, benzimidazoles such as Fenbendazole, Mebendazole or Albendazole seem to be safe drugs.
However, a drug without any side-effects does not exist. Scientific data reports do not reveal significant adverse reactions from taking fenbendazole. Despite the fact, there are anecdotal reports of potential toxicity: Up to 5 % of people can experience stomach discomfort or diarrhea when taking large quantities of fenbendazole with no breaks.
People with severe liver or kidney failure have lower medication excretion rates, therefore, fenbendazole can accumulate and cause unexpected side-effects. Doses should be divided accordingly in this situation.
When used in large quantities for a long period of time without breaks, fenbendazole can cause an asymptomatic liver enzyme increase due to the fact of the substance being mainly metabolized in the liver. This is reversible with the help of a couple week pause from the medication.
Therefore, patients should get a blood panel that includes the liver enzymes of AST, ALT, Alkaline Phosphatase, before taking Fenbendazole. Liver enzymes may also be elevated from cancer treatments, alcohol use, certain medications, and cancer itself.
Elevated liver enzymes indicate a liver that is stressed and inflamed, and adding to its burden with Fenbendazole would not be recommended.
Generally, for those with normal lab values, after one month of Fenbendazole treatment, patients should get a comprehensive metabolic panel (CMP). This standard blood test will check the liver and kidney function to assure that the patient is tolerating Fenbendazole without any concerning impacts on the vital organs.
The protocol was designed to keep the liver in optimal health, therefore the schedule of weekly 3 days on, 4 days off was previously suggested. However, more and more people are using fenbendazole on a daily basis without problems.
We would still recommend taking at least 1 day off per week to avoid over stressing the liver if the medication is to be used for prolonged periods of time (like months or years).
Both fenbendazole and mebendazole have favorable safety profiles with low toxicity. However, caution is advised:
Liver Function: Elevated liver enzymes have been reported; patients with liver disease should be closely monitored.
Gastrointestinal Effects: Up to 5% of users may experience mild stomach discomfort or diarrhea, especially at high doses.
Drug Interactions: Co-administration with drugs like metronidazole may cause severe adverse reactions.
Regular monitoring of liver enzymes and kidney function is essential during treatment.
Chapter 5: Niclosamide for Cancer
Background
Niclosamide is an FDA-approved antihelminthic drug first developed by Bayer in the late 1950s and approved for human use in 1962 under the brand name Yomesan. Chemically classified as a chlorinated salicylanilide, it has been used safely for decades to treat intestinal tapeworm infections. Unlike fenbendazole, it already carries an established human approval — a meaningful head start for off-label oncology use.
In recent years, high-throughput drug screening campaigns have repeatedly and independently flagged niclosamide as a potent anticancer compound. A 2025 comprehensive review in the European Journal of Medicinal Chemistry described it as “a multi-targeted therapeutic agent” with compelling effects across a wide range of malignancies, including drug-resistant leukemia, ovarian cancer, colorectal cancer, prostate cancer, and oral cancers.
Its main clinical barrier is poor oral bioavailability — the drug is only partially absorbed from the gastrointestinal tract at standard doses, making it difficult to achieve the serum concentrations needed for systemic anticancer effect. This is an active area of research, with novel formulations, prodrug derivatives, and nanotechnology-based delivery systems all under investigation.
How Niclosamide May Fight Cancer
Niclosamide’s anticancer profile is unusually broad. Unlike many targeted agents that act on a single pathway, niclosamide simultaneously disrupts multiple oncogenic signaling networks:
Wnt/β-catenin inhibition: Niclosamide suppresses this pathway by degrading the LRP6 co-receptor and reducing the expression of downstream targets including β-catenin, Cyclin D1, and c-Myc — all of which cancer cells depend on for proliferation and stem cell maintenance.
STAT3 inhibition: STAT3 is a key driver of tumor survival, immune evasion, and resistance to therapy. Niclosamide suppresses STAT3 signaling across multiple cancer types, reducing cancer cell proliferation and enhancing sensitivity to other treatments.
mTORC1 inhibition: By blocking mTOR complex 1, niclosamide impairs protein synthesis and metabolic activity in rapidly dividing cancer cells.
NF-κB inhibition: NF-κB drives inflammation-related tumor growth and resistance to apoptosis. Niclosamide suppresses this pathway, promoting cancer cell death.
Notch inhibition: The Notch pathway is a key regulator of cancer stem cell self-renewal. Niclosamide’s suppression of Notch signaling is particularly relevant to preventing tumor recurrence.
Mitochondrial uncoupling: Perhaps its most distinctive mechanism, niclosamide acts as a protonophore — it dissipates the mitochondrial proton gradient, converting it to heat rather than ATP. This deprives cancer cells of their primary energy source and induces metabolic stress leading to cell death. Normal cells appear more tolerant of this effect.
Cancer stem cell inhibition: Niclosamide consistently ranks among the most potent inhibitors of cancer stem cells identified in drug screening programs. Cancer stem cells are responsible for tumor initiation, metastasis, and recurrence after treatment — making their suppression a critical therapeutic goal.
Ferroptosis induction: Recent studies (Mathew et al., 2024) have shown that niclosamide can simultaneously modulate multiple ferroptosis-related mechanisms, adding another cell-death pathway to its arsenal.
Epithelial-to-mesenchymal transition (EMT) inhibition: Niclosamide reduces cancer cell migration and invasion by upregulating E-cadherin and TIMP2 while suppressing vimentin, snail, MMP2, and MMP9 — proteins that cancer cells use to break through tissue barriers and spread.
Overcoming multidrug resistance: Preclinical evidence shows niclosamide can restore sensitivity to drugs in resistant leukemia and ovarian cancer models.
Cancer Types with Preclinical Evidence
Niclosamide has demonstrated activity across a wide range of tumors in cell culture and animal models:
Colorectal cancer: One of the most studied indications. Niclosamide suppresses Wnt/β-catenin-driven metastasis via S100A4, and inhibits tumor growth in xenograft models. This led directly to the NIKOLO clinical trial.
Prostate cancer (castration-resistant): Niclosamide inhibits androgen receptor splice variants and FOXM1-mediated DNA damage response pathways that drive castration resistance. It reduced xenograft tumor growth in vivo in multiple studies.
Breast cancer: Identified in drug screening as a potent inhibitor of breast cancer stem-like cells. Active in triple-negative breast cancer (TNBC) models through ferroptosis modulation and STAT3 inhibition.
Ovarian cancer: Shows activity in platinum-resistant ovarian cancer models and synergizes with standard agents.
Oral squamous cell carcinoma (OSCC): Inhibits cancer stem cell populations, reverses EMT, and enhances cisplatin sensitivity.
Leukemia: Effective in multidrug-resistant leukemia models, overcoming efflux-based resistance mechanisms.
Lung, pancreatic, and hepatic cancers: Preclinical activity documented; fewer published studies than in colorectal and prostate cancer.
Inhibitory concentrations (IC50) for most cancer cell lines tested have been less than 1 μM — a concentration that, while currently difficult to achieve with standard oral dosing, is theoretically accessible with improved formulations.
Clinical Evidence and Trials
Niclosamide’s transition to clinical oncology has been slowed primarily by the bioavailability problem. Key trials to date:
NIKOLO Trial (NCT02519582) — Colorectal Cancer, Phase II: Patients with metastatic CRC progressing after standard therapy received 2 g of niclosamide orally once daily until disease progression. The trial was designed to assess progression-free survival at 4 months, overall survival, disease control rate, and niclosamide plasma concentrations. Results have been instructive: the trial confirmed biological rationale but highlighted the pharmacokinetic challenges of achieving therapeutic systemic levels with oral tablets.
NCT02687009 — Colon Cancer, Phase I: Evaluated niclosamide safety in patients with resectable colon cancer before surgery, using three escalating dose levels. The trial was terminated due to low accrual.
NCT02532114 — Castration-Resistant Prostate Cancer, Phase I: Tested oral niclosamide combined with enzalutamide. The maximum tolerated dose was 500 mg three times daily, and plasma concentrations did not consistently reach the threshold needed to inhibit CRPC growth in preclinical models. The Data Safety Monitoring Board closed the trial early. No PSA decline was observed.
Hyundai Bioscience (2024): Announced a clinical development plan for an oral niclosamide metabolic anticancer drug specifically targeting p53-mutant cancers — one of the most common and treatment-resistant mutation profiles in oncology, affecting ovarian, uterine, and esophageal cancers among others.
The overall picture from clinical trials is that unmodified oral niclosamide does not reliably achieve anticancer plasma concentrations. This has redirected research toward:
Novel salt forms (niclosamide ethanolamine, niclosamide piperazine) with improved water solubility
Prodrug derivatives such as PDMX1001 (niclosamide acetate), currently entering trials for CRPC
Nanotechnology-based delivery systems including nanostructured lipid carriers (NLC) and electrosprayed nanoparticles
Alternative delivery routes including rectal suppositories, which may bypass first-pass hepatic metabolism
Dosing Considerations
Standard antiparasitic dosing of niclosamide (typically 2 g as a single dose, or 2 g/day for several days) is well tolerated but does not achieve anticancer plasma concentrations with conventional oral tablets. The maximum tolerated dose in oncology trials has been 500 mg three times daily — still pharmacokinetically insufficient for most tumor types.
Pediatric antiparasitic dosing (0.3–1.2 mg/kg/day) is well tolerated with an excellent safety profile, which has made niclosamide attractive for exploration in pediatric oncology.
For patients considering off-label use, meaningful systemic exposure with standard tablet formulations is not assured. The most promising near-term options are improved formulations, where available, or combination with agents that may enhance niclosamide’s local or systemic effects.
Safety Profile
Niclosamide has a favorable safety record developed over more than 60 years of antiparasitic use. At standard therapeutic doses, side effects are minimal and typically limited to mild gastrointestinal symptoms (nausea, abdominal discomfort). At higher doses used in oncology trials (up to 500 mg three times daily), tolerability has generally been acceptable, with no unexpected serious adverse events reported.
The drug’s poor oral bioavailability — while a pharmacokinetic limitation — also acts as a natural safety buffer: systemic exposure at standard oral doses remains low, limiting off-target effects.
Key consideration: The main challenge with niclosamide is not toxicity but efficacy — achieving tumor concentrations high enough to activate its anticancer mechanisms with standard oral administration. Formulation improvements are the critical next step before niclosamide can be meaningfully incorporated into clinical protocols.
Chapter 6: Updated Joe Tippens Protocol
The following is a modernized version of the original Joe Tippens protocol, updated to incorporate the ivermectin- and mebendazole-based regimen published in the Journal of Orthomolecular Medicine (2024). It combines repurposed antiparasitic drugs with evidence-supported nutraceuticals:
Ivermectin - 24 mg daily (6 days per week), or up to 1 mg/kg/day for aggressive or advanced cancers. Take with a high-fat meal to maximize absorption.
Mebendazole — 200–400 mg daily. Alternatively, fenbendazole at 300 mg six days per week, with doses up to 1 gram per day for aggressive cancers.
Vitamin D - 62.5 mcg [2500 IU] daily, seven days a week.
Bio-Available Curcumin - 600 mg per day, 7 days a week.
Enhanced absorption Berberine - 500 mg per day, to help limit glucose availability to cancer cells.
Diet and Lifestyle:
Eliminate or sharply limit added sugars (the BMJ 2023 umbrella review recommends keeping free/added sugars below 25 g/day and reducing sugar-sweetened beverages to fewer than one per week).
Follow a whole-food diet and minimize ultra-processed foods (per BMJ 2024 guidelines).
Prioritize adequate sleep and effective stress management.
Protocol Notes:
Vitamin E: Removed from the protocol (Joe Tippens, July 22, 2020) due to interactions (e.g., with blood thinners).
Ivermectin can significantly increase the blood-thinning effect of warfarin (Coumadin), and combining them increases the risk of dangerous or unusual bleeding. It may also interact with other anticoagulants, and patients should be closely monitored by a physician.
This protocol is not a replacement for standard oncology care. It is designed as an adjunct strategy to complement, not replace, conventional treatment.
Conclusion and Future Directions
Ivermectin, fenbendazole, mebendazole, and niclosamide have each emerged from the antiparasitic toolkit as compelling candidates for drug repurposing in cancer. Their ability to disrupt cancer cell metabolism, induce multiple forms of cell death, and overcome drug resistance offers hope for affordable, accessible cancer treatments.
We acknowledge that double-blind, prospective, randomized controlled trials (RCTs) are the current gold standard in medical research. However, N=1 trials, open-label studies, personalized medicine and real-world data offer practical alternatives. While these approaches are less rigorous than RCTs—which are costly and time-consuming—they can still provide valuable insights, particularly for rare or advanced cancers. That said, their limitations, such as the absence of control groups and potential bias, must be carefully considered.
For patients with Stage 4 or aggressive cancers, exploring all available options is crucial given the high-stakes risk-benefit ratio. In that context, the “off-label” usage and "right to try" carries genuine moral weight.
Clinical guides are based on research, but not every clinical decision is solely research-driven. A personalized clinical approach can also be viewed as a series of N=1 trials, where multiple interventions are tested within the same individual. By integrating empirical evidence, clinical observations, and objective assessments—such as cancer markers and PET scans—doctors can closely monitor and observe both the effectiveness and safety of treatments almost immediately.
Ivermectin, Fenbendazole and Mebendazole offer promising, yet experimental, cancer treatment options. While clinical trials remain limited, emerging studies suggest promising applications across multiple cancer types. Patients should consult healthcare professionals before considering these protocols.
The momentum is undeniable. However, fenbendazole and ivermectin are not magic bullets. They may have a place as pieces in your larger anti-cancer strategy. But cancer rarely succumbs to one or two interventions, however determined.
True empowerment comes from multi-layered action. Keep conversations open with professionals experienced in repurposing and metabolic approaches. You’re not alone—keep asking the hard questions, keep fighting smart, keep trying.
What is needed now:
Optimized formulations of niclosamide to achieve reliable therapeutic plasma concentrations — this is the single most important bottleneck for its clinical translation.
Well-designed randomized controlled trials, or pragmatic trial designs suited to the complexity of advanced cancer, for all four agents.
Research into combination regimens involving immunotherapy, metabolic interventions (ketogenic diets, GLP-1 agonists), and these antiparasitic agents.
Mechanistic studies on these drugs’ effects in drug-resistant tumors and the tumor microenvironment.
Investigation of synergies between niclosamide and the benzimidazoles (fenbendazole, mebendazole), given their complementary but non-overlapping mechanisms.
These are not fringe ideas. They are legitimate scientific questions deserving of legitimate scientific resources.
Cancer rarely yields to one or two interventions, however promising. True empowerment for patients comes from a multi-layered strategy — antiparasitic repurposed drugs as one piece, alongside metabolic support, immune optimization, and open collaboration with clinicians familiar with integrative approaches.
As the evidence continues to grow, so does the obligation to take it seriously.
This article is part of the ivermectin and fenbendazole series. Explore other popular articles related to this series:

Ivermectin and mebendazole, both approved for human use, are now available in the U.S.
Researched and approved by Dr. Peter McCullough.
Prescribed by licensed medical professionals
Compounded and dispensed by a licensed US-based pharmacy
Approved for human use
Lab-tested for potency, with doctor consultation included and free U.S. shipping.
99 of 106 verified reviewers gave the combo 5 stars.
Where to buy Ivermectin and Mebendazole Formula: Available on The Wellness Company's website. Here is the link: Ivermectin and Mebendazole.
If pharma makes them, do I still trust them? Not really. I’ll stick with CDS, (Chlorine Dioxide).